Request Appointment
Enter your details and we will be in touch with you shortly;
Or call
8655885566
between 8 am and 8 pm.




Trunk muscle dysfunction and weakness is an important risk factor for developing low back pain (LBP).1–3 Trunk muscle strength compensates for dysfunction due to LBP, and reduced trunk range of motion (RoM) and muscle strength can lead to functional limitations and disability in subjects with LBP.2,4 Hence, restoring trunk muscle strength and RoM using exercises helps reduce pain and disability, improve function, and prevent recurrence in patients with LBP.5 Furthermore, improvement in the trunk or lumbar RoM and strength is a useful parameter to measure the effectiveness of rehabilitation treatment in patients with LBP.6,7 Hence, measuring trunk RoM and isometric strength (IS) in a patient with LBP will help quantify deficits in trunk RoM and strength, individualize rehabilitation treatment based on these deficits, and record improvement with treatment.
Baseline paraspinal muscle strength and trunk mobility may vary based on the subject characteristics, such as gender, age, duration of symptoms, pain intensity, and disability on presentation.1,8–10 Previous studies on trunk RoM and IS evaluated specifically lumbar or trunk extensor muscle strength rather than global trunk RoM and IS and measured these parameters in a group with a broad range of age.1,8–10
To the best of our knowledge, no studies in the literature have specifically investigated the difference in trunk RoM and IS between symptomatic and asymptomatic subjects in the vulnerable 20 to 40 years age group and investigated gender-based difference in trunk RoM and IS between symptomatic with LBP and asymptomatic subjects in this age group. We believe that determining gender-specific variations in trunk RoM and IS parameters will help design patient-specific rehabilitation treatment protocols based on these deficits in patients undergoing conservative management of LBP. Hence, this study aimed to compare trunk RoM and IS in subjects with LBP and similar asymptomatic subjects, compare trunk RoM and IS in symptomatic and asymptomatic subjects in males and females, and determine factors that influence trunk RoM and IS in the symptomatic and asymptomatic groups.Wehypothesized that therewould be a significant difference between symptomatic and asymptomatic subjects, both in males and females, in terms of trunk RoM and IS.
The present prospective comparative study was conducted at a chain of outpatient clinics specializing in spine rehabilitation (QI Spine Clinic, India) from April 2019 to March 2020. Participants were divided into symptomatic LBP (case) and asymptomatic (control) groups and compared in this study. The study protocol was approved by an institutional review board and ethics committee, and all participants signed and informed consent form for participation in this study.
Subjects in the symptomatic (LBP) group were recruited from patients who came for evaluation of their LBP and underwent trunk RoM and IS testing at one of our three spine rehabilitation outpatient clinics in one city. A total of 149 consecutive subjects with LBP who underwent trunk RoM and IS testing during the study period were eligible for participation in the symptomatic group. Asymptomatic subjects were recruited among the relatives of patients in the symptomatic group and among the physical therapists working at any of our 8 spine rehabilitation clinics in 3 cities. A total of 84 asymptomatic volunteers who consented to trunk RoM and IS testing were eligible for participation in the study as part of the asymptomatic group.
The inclusion criterion for the symptomatic group was patients who presented at the clinic for evaluation of mechanical LBP. The exclusion criteria were patients < 20 years or > 40 years of age, peripheral joints involvement, structural kyphotic or scoliotic deformities, previous spine surgery, and incomplete clinical records. The inclusion criterion for the asymptomatic group was participants without LBP or any musculoskeletal symptoms within the last year. The exclusion criteria for the asymptomatic group were patients < 20 years or > 40 years of age, history of spine trauma, spine tuberculosis, or kyphotic/scoliotic deformities.
After recording the clinical history, all subjects were examined for posture, lumbar RoM, straight leg raising (SLR) test, and myotomal and dermatomal function. Based on history and examination, subjects with LBP were diagnosed with mechanical LBP if the pain arose from the spine, intervertebral discs or surrounding soft tissues, worsened with specific spine movement, and improved with rest.11 Pain in the symptomatic group was measured using the numerical pain rating scale (NPRS) score.12
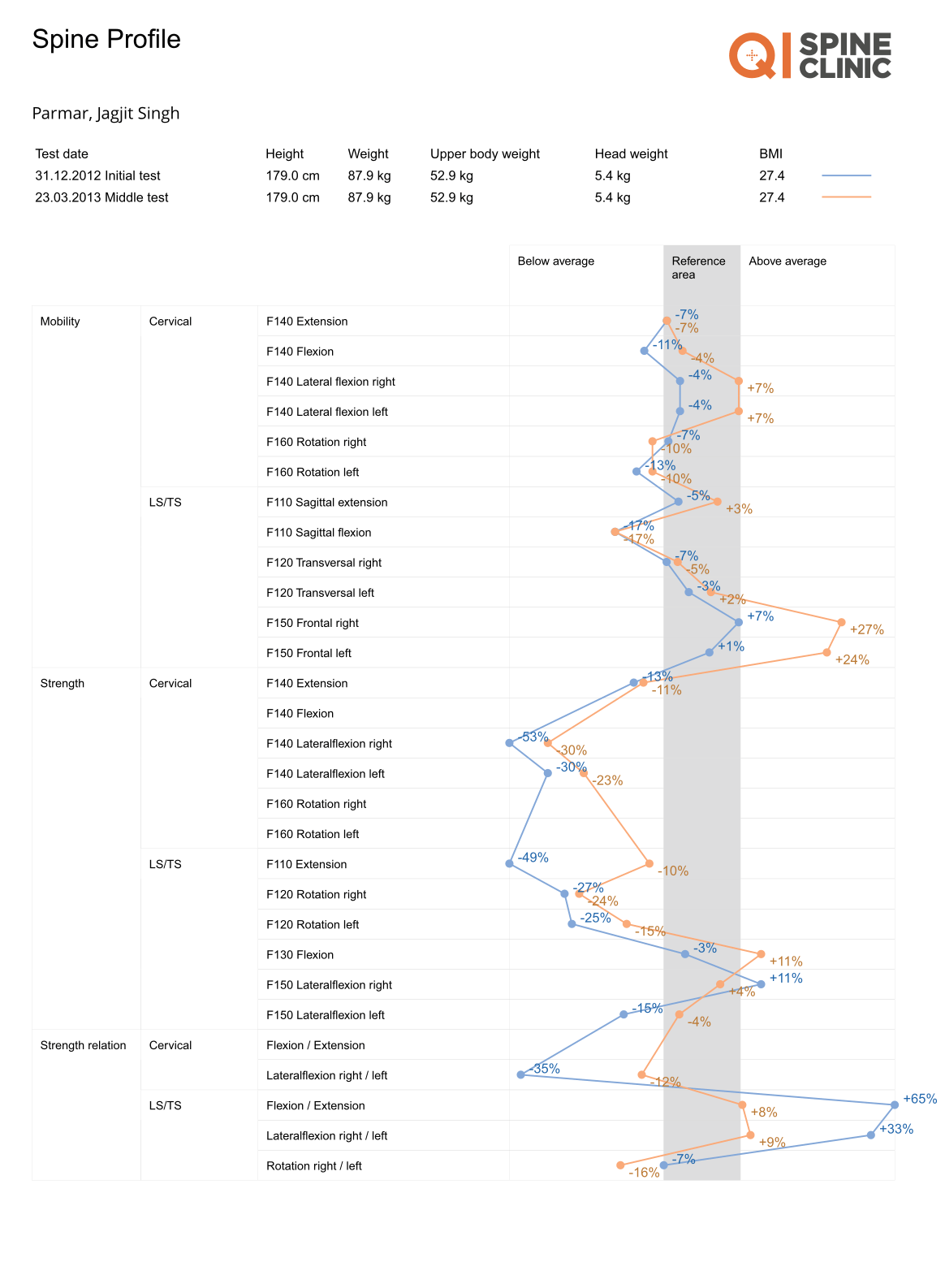
Trunk RoM and IS were tested in all subjects using a dynamometer-based equipment using a protocol previously described.13 Good-to-excellent reliability and reproducibility of ITS testing using this device has been reported previously.13All participants were tested on 3 separate devices (for extension, flexion, and rotation) in the seated position and fastened in place using a knee-lock system and a thigh restraining belt that immobilized the hip and thigh and allowed movement only at the lower back and trunk. To begin testing, the trunk was locked at 30° flexion from the upright sitting position for extension, placed in a neutral position for flexion, and the lower body laterally rotated 30° in the transverse plane for rotation and confirmed visually on the screen of the device. After initial warm-up, all participants generated their maximum isometric attempts was stored. Intervals between maximum test repetitions or attempts were a minimum of 15 seconds. The 3 different maximum isometric tests (extension, flexion, and rotation) were separated by 5 minutes. The entire strength evaluation was performed under the supervision of a spine physiotherapist trained and experienced in the use of the equipment. Trunk RoM was measured on all three devices sequentially after finishing the specific ITS testing. Both strength (torque) and motion values (degrees) were captured by the device software and stored in its server contraction by gradually increasing their torque moment up to their maximum within the first 2 to 3 seconds of each contraction. The best value obtained out of 3 attempts was stored. Intervals between maximum test repetitions or attempts were a minimum of 15 seconds. The 3 different maximum isometric tests (extension, flexion, and rotation) were separated by 5 minutes. The entire strength evaluation was performed under the supervision of a spine physiotherapist trained and experienced in the use of the equipment. Trunk RoM was measured on all three devices sequentially after finishing the specific ITS testing. Both strength (torque) and motion values (degrees) were captured by the device software and stored in its server.
Demographic data, including gender, age, body mass index (BMI), lifestyle, and duration of symptoms (acute/ subacute < 12 weeks, chronic 12 weeks), were collected from all participants. For trunk RoM, maximum extension, flexion, right rotation, and left rotation were recorded in degrees. For ITS, maximum torque for trunk extension, flexion, right rotation, and left rotation were recorded in Nm. The extension-flexion RoM ratio was calculated by dividing the maximum extension RoM value (degrees) by the maximum flexion RoM value (degrees), and the extensionflexion strength ratiowas calculated by dividing themaximum extension strength value (Nm) by the maximum flexion strength value (Nm) to determine extension-flexion RoM and ITS imbalance
Based on mean isometric flexion muscle strength findings in an initial pilot test of 10 subjects, for a 20% difference in isometric flexion muscle strength between the 2 groups, an α value of 0.05 with power at 80%, a minimum sample size of 63 subjects was calculated in each group using the ClinCalc sample size calculator (ClinCalc LLC, Indiana, USA). Categorical data were compared using the Chi-squared test, and continuous data were compared using one-way analysis of variance (ANOVA) between the symptomatic and asymptomatic groups and gender-based subgroups. A multivariate analysis was performed to determine the effect of age, gender, BMI, lifestyle, and symptom duration on extension and flexion trunk RoM and IS in both asymptomatic and symptomatic subjects. A pvalue < 0.05 was considered significant. Statistical analysis was performed using the GraphPad QuickCalcs online statistical analysis tool (GraphPad Software, San Diego, CA, USA).
Based on the exclusion criteria, 76 subjects were excluded from the symptomatic LBP group (12 subjects with incomplete clinical records and 64 subjects who were outside the 20–40 years age group) and 4 subjects were excluded from the asymptomatic or control group (1 subject with a historyof spinal tuberculosis and 3 subjects who were outside the 20–40 years age group). Hence, data from 73 subjects in the symptomatic LBP group (40 males and 33 females) and 80 subjects in the asymptomatic group (24 males and 56 females) were analyzed. Characteristics of all subjects are summarized in ►Table 1.

In males, the mean trunk extension RoM was significantly lower (p< 0.0001) in symptomatic subjects when compared with asymptomatic subjects (►Table 2 and ►Fig. 1), and the mean trunk extension (p< 0.0001), flexion (p< 0.0001), and rotation (p< 0.0001) strengths were significantly lower in symptomatic subjects when compared with asymptomatic subjects (►Table 2 and ►Fig. 2). However, the mean flexion and rotation ROMs, and the mean extension-flexion RoM (p¼ 0.09) and mean extensionflexion strength (p¼ 0.55) ratios were not significantly different between the 2 subgroups (►Table 2 and ►Fig. 1).
Comparison of Trunk RoM and IS in Symptomatic and Asymptomatic FemalesIn females, the mean trunk flexion RoM was significantly lower in symptomatic subjects when compared with asymptomatic subjects (►Table 2 and ►Fig. 1). The mean extension-flexion RoM (p ¼ 0.04) and mean extension-flexion strength (p ¼ 0.04) ratios were significantly greater in symptomatic subjects when compared with asymptomatic subjects. However, there was no significant difference for mean trunk extension RoM and rotation RoM and mean trunk extension, flexion, and rotation strengths between the two subgroups (►Table 2 and ►Figs. 1, 2).
Factors Affecting Trunk RoM and IS in Asymptomatic and Symptomatic SubjectsIn asymptomatic subjects, multivariate analysis showed that female gender and higher BMI were significantly associated with less trunk extension RoM, whereas no factors were found to significantly affect flexion RoM (►Table 3). For ITS, female gender and lower BMI were significantly associated with less trunk extension strength, whereas female gender was significantly associated with less trunk flexion strength (►Table 3). In subjects with LBP, the multivariate analysis showed that no factors significantly affected extension and flexion RoM, whereas female gender and higher age were significantly associated with less extension ITS, and female gender alone was significantly associated with less flexion ITS (►Table 4).
The results of this study indicate that although symptomatic males had significantly less mean trunk extension RoM and mean trunk IS compared with asymptomatic males, there was no significant difference in trunk extension RoM and IS when asymptomatic and symptomatic females were compared. However, the mean extension-flexion RoM and mean extension-flexion ITS ratios in females were significantly lower in asymptomatic subjects when compared with symptomatic females. Female gender was significantly associated with less extension and flexion ITS in both symptomatic and asymptomatic subjects
A previous gender-based comparison between symptomatic and asymptomatic subjects showed no difference in extensor ITS in males, whereas it was significantly higher in asymptomatic females when compared with females with chronic LBP.8 These findings are contrary to the results of the current study. This could be explained by a higher number of subjects in the symptomatic group, a broader age range of the study population (18–90 years), inclusion of only chronic LBP, and recruitment of asymptomatic subjects mainly from the general community in their study.8
In contrast to male subjects, no significant difference was found in trunk extension RoM and ITS between asymptomatic and symptomatic female subjects in the current study. Similarly, in contrast to male subjects, the mean extensionflexion RoM and mean extension-flexion strength ratios in females were significantly lower in asymptomatic subjects when compared with symptomatic subjects. The extensionflexion strength ratio indicates an increased antagonist/agonist imbalance, and a higher ratio signifies less flexors’ ITS relative to extensors’ ITS. Hence, this finding indicates that in female subjects with LBP, weakness of individual trunk extension or flexor muscle groups may be less of an issue than an imbalance between the trunk extensors and flexors. Trunk strength imbalance is seen in LBP and has been reported to increase the risk of injury and pain during functional activities in subjects with LBP.14,15 A significant increase in flexion-extension peak torque ratio in symptomatic subjects compared with asymptomatic subjects in both males and females has been reported.15 This highlights the need for correcting extension-flexion strength imbalance by trunk flexor/abdominal muscle (e.g., transversus abdominis) strengthening vis-à-vis extensor muscles (e.g., multifidus, erector spinae) in women with LBP. Furthermore, lack of difference in ITS between asymptomatic and symptomatic females, in contrast to males, indicates that weak individual muscle groups may not be a cause or underlying pathology of LBP in women, and other factors such as BMI and genetic factors may play a role in them.16,17
The multivariate analysis showed that female gender and higher BMI were significantly associated with less trunk extension RoM in asymptomatic subjects. Although the female gender has been reported to have greater joint RoMs than males,18 our findings indicate that this may not be true for extension RoM. For ITS in asymptomatic subjects, the female gender was significantly associated with less extension and flexion ITS. A previous study confirmed these findings, which reported a significant correlation between female gender and lesser extensor and flexor ITS in young adults.19 Pajoutana et al.16 reported no significant correlation between extensor ITS and increased BMI or trunk fat mass in asymptomatic young adults, which were contrary to the findings of our study. However, obese individuals may have significantly higher trunk extensor and flexor torque, which could be due to the additional body mass acting as a loading and training stimulus on the anti-gravity trunk extensors.20,21 Female



gender and increasing age as risk factors for weak extensor and flexor ITS in LBP have not been previously reported in young adults. However, a significant association between female gender and increasing age and trunk muscle weakness has been reported in older adults.22
The current study has a few limitations. First, asymptomatic subjects were recruited using a convenience sampling method, which may have caused selection bias, and, hence, our findings should be replicated using controls from the general population. Secondly, the maximum effort applied by symptomatic subjects during trunk RoM and ITS testing might be affected by patient’s fear-avoidance behavior and pain tolerance rather than their muscle function. However, to avoid this, we ensured that all symptomatic patients were tested after their pain has reduced to NPRS < 3, and the best of 3 RoM and ITS readings were recorded. Finally, despite determining correlation of factors such as gender and BMI with RoM and ITS variations, the underlying structural or pathological reason for reduced RoM and ITS in patients with LBP could not be determined from the data collected in the current study. However, previous studies have reported various factors such as differences in trunk muscle size and recruitment patterns,23 muscle strength, endurance and force control,10 and lumbopelvic kinematics,14 as probable causes of the difference in RoM and ITS between subjects with or without LBP.
Males with LBP had significantly weaker extensor, flexor, and rotator ITS when compared with asymptomatic males. Although there was no significant difference in ITS in symptomatic versus asymptomatic females, LBP caused significant extension-flexion RoM and ITS imbalance indicating that flexors were weaker than the extensor muscle groups in females. In both symptomatic and asymptomatic subjects, the female gender was significantly associated with weak extensor and flexor ITS. These gender-based variations in trunk RoM and IS, especially the extensor-flexor IS imbalance in females, must be considered while designing rehabilitation treatment protocols for LBP.
Financial Support
There was no financial support from public, commercial, or non-profit sources.
Conflict of Interests
The authors have no conflict of interests to declare.
Visit our nearest clinic for your first consultation